| The Antidepressant Waiting Game |
 |
Part 1: The Chemistry of Depression By Nancy Schimelpfening
Even after one works up the courage to seek help, finding an antidepressant or combination of antidepressants that relieves the depression without unbearable side-effects can a frustrating proposition. Each medication requires a trial of several weeks before it can be declared ineffective and another tried. Several trials may be required to fine tune your medications. Some unlucky individuals may hang on for literally years without a satisfactory solution being found.
So why can't your doctor just write a prescription for Prozac and send you on your way to live happily ever after? In coming weeks, we are going to take a look at this problem by examining what we know about the neurobiology of depression, how antidepressants work, how doctors currently go about matching antidepressants with your needs, why getting treated by your family doctor can hinder your progress, and what the future may hold for depression treatments.
Brain Chemistry Basics
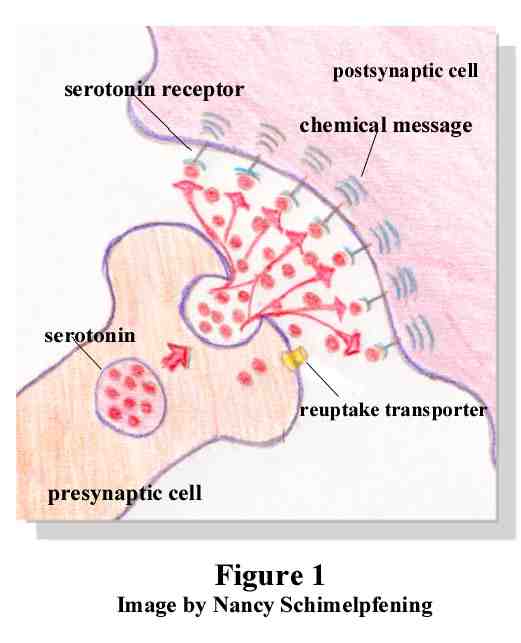
You've probably probably heard the term "neurotransmitter" before, but what does this really mean? Neurotransmitters are chemical messengers within the brain that facilitate communication between nerve cells. Let's illustrate with serotonin. Figure 1 depicts the junction between two nerve cells. Packets of serotonin molecules are released from the end of the presynaptic cell (the axon) into the space between the two nerve cells (the synapse). These molecules may then be taken up by serotonin receptors of the postsynaptic nerve cell (the dendrite) and thus pass along their chemical message. Excess molecules are taken back up by the presynaptic cell and reprocessed.
Several things might potentially go wrong with this process and lead to a serotonin deficit. Just to enumerate a few possibilities:
-
Not enough serotonin is produced,
-
There are not enough receptor sites to receive serotonin,
-
Serotonin is being taken back up too quickly before it can reach receptor sites,
-
Chemical precursors to serotonin (molecules that serotonin is manufactured from) may be in short supply, or
-
Molecules that facilitate the production of serotonin may be in too short supply.
As you can see, if there is a breakdown anywhere along the path, neurotransmitter supplies may not be adequate for your brain's needs. Inadequate supplies lead to the symptoms that we know as depression.
The Primary Players
There are three basic molecules, known chemically as monoamines, which are thought to play a role in mood regulation: norepinephrine, serotonin and dopamine.
In the 1960s Joseph J. Schildkraut of Harvard University cast his vote with norepinephrine as the causative factor for depression in the now classic "catecholamine" hypothesis of mood disorders. He proposed that depression stems from a deficiency of norepinephrine in certain brain circuits and that mania arises from an overabundance of this substance.1 There is indeed a large body of evidence2 that supports this hypothesis, however, changes in norepinephrine levels do not affect mood in everyone. The implication is that medications such as reboxetine, which specifically targets norepinephrine, will work for some persons but not others.3
Obviously there must be some other factor that interacts with norepinephrine to cause depression. Serotonin has been found to be this other factor. This molecule has taken center stage in the past two decades thanks to Prozac and other Selective Serotonin Reuptake Inhibitors (SSRI's), which selectively act on this molecule. Serious investigations into serotonin's role in mood disorders, however, have been going on for almost 30 years, ever since Arthur J. Prange, Jr., of the University of North Carolina at Chapel Hill, Alec Coppen of the Medical Research Council in England and their co-workers put forward the so-called "permissive hypothesis". This view held that synaptic depletion of serotonin was another cause of depression, one that worked by promoting, or "permitting," a fall in norepinephrine levels. So, although, norepinephrine still played a major role in depression, serotonin levels could be manipulated to indirectly raise norepinephrine. Newer antidepressants like Effexor are actually targeted at both serotonin and norepinephrine.4 Tricyclics (TCAs) also affect both norepinephrine and serotonin, however, they have the added effect of influencing histamine and acetylcholine, which produces the side-effects that TCAs are known for, such as dry mouth or eyes, peculiar taste in mouth, sensitivity to light of the eyes, blurry vision, constipation, uninary hesitancy, and others. SSRIs do not affect histamine and acetylcholine and thus do not have the same side-effects as the older medications.5
A third substance that may play a role in mood is dopamine. Dopamine is associated with the reward, or reinforcement, that we get which causes us to continue participating in an activity. It has been implicated in such conditions as Parkinson's Disease and schizophrenia. There is also some evidence that, at least for a subset of patients, dopamine plays a role in depression.6 Dopaminergic substances and stimulants have been used as antidepressants when other measures have failed.7 Some studies have investigated dopaminergic agents as a rapid method of relieving depression (in contrast to medications which may take up to six weeks to exhibit their full effect).8
Although agents that work selectively on dopamine have the benefit of fast action, they have also exhibited some properties which have kept them from being as widely used as other antidepressants. Dopamine is a neurotransmitter that is associated with addiction and it's production is stimulated by drugs such as cocaine, opiates and alcohol (which may explain why depressed persons choose to self-medicate with drugs and alcohol.9) Drug specifically targeted at dopamine, for example amineptine (Survector), present the potential for abuse.10 For this reason, amineptine is not approved for use in the US or Britain at this time.

 Important Announcement
Important Announcement

 First
First 