|
|
 |
 First
Previous
2-8 of 8
Next First
Previous
2-8 of 8
Next Last
Last
|
|
Reply
| | | From: Joel | Sent: 7/12/2006 10:18 PM |
From the American Cancer Society | When Smokers Quit—The Health Benefits Over Time |  | | 20 minutes after quitting: Your blood pressure drops to a level close to that before the last cigarette. The temperature of your hands and feet increases to normal. 8 hours after quitting: The carbon monoxide level in your blood drops to normal. 24 hours after quitting: Your chance of a heart attack decreases. 2 weeks to 3 months after quitting: Your circulation improves and your lung function increases up to 30%. 1 to 9 months after quitting: Coughing, sinus congestion, fatigue, and shortness of breath decrease; cilia (tiny hair like structures that move mucus out of the lungs) regain normal function in the lungs, increasing the ability to handle mucus, clean the lungs, and reduce infection. 1 year after quitting: The excess risk of coronary heart disease is half that of a smoker's. 5 years after quitting: Your stroke risk is reduced to that of a nonsmoker 5-15 years after quitting. 10 years after quitting: The lung cancer death rate is about half that of a continuing smoker's. The risk of cancer of the mouth, throat, esophagus, bladder, kidney, and pancreas decrease. 15 years after quitting: The risk of coronary heart disease is that of a nonsmoker's.
| |
|
Reply
| | | From: Joel | Sent: 7/12/2006 10:19 PM |
“I have smoked for so long and so much, what is the use in quitting now?�?/EM>
On the third day of a recent clinic, a woman participant in her late fifties who had been off smoking for just over 48 hours asked one of those questions that I have heard hundreds of times in past programs. “I have smoked so long and so heavily, what good will quitting smoking do for me now?�?nbsp; A few minutes of explaining the bargaining phase people go through when they are initially quitting smoking seemed to clarify why she was having such thoughts rationalizing why she didn’t really need to quit. A few minutes later, she told me a story about her personal family history, one that quite simply gave a better answer to her original query than I could ever have come up with. “My father was a chain smoker,�?she said. “He quit when he was 60 because he had a heart attack. Never smoked one after that. Even though he was a heart attack victim, after he quit smoking he felt better than he had felt in years. Much more endurance, greater vitality. He lived to the age of 95, bright and alert to the end.�?/FONT> On the sixth night I called her to see if she had made it through the weekend all right. “I feel so bad,�?she replied. “I had a terrible evening last night and I had a major problem dealing with a client at work this morning. I was just so upset from lack of sleep and frustration, I finally broke down and took a cigarette. I’ve been beating myself up for it ever since. I am more depressed now than I was before. Why am I beating myself up so, and what should I do now?�?/FONT> I said she had two options, quit right then and face a potential full three day withdrawal or go back to full fledged smoking all over again. If she didn’t make a decision, her body would automatically make the decision for her. Again she expressed the sentiment that she was beating herself up so badly and wanted me to explain why she was so upset with herself. She just couldn’t believe that one cigarette could be so important to be making such a big issue. A few minutes later, she told me the story of how her husband had once been off for three years. One day while they were in the car together, for one reason or another he bummed a cigarette from her. She raised the issue with him of what good would a cigarette be after all that time, but he convinced her it was no big deal. What right did she have to protest anyway, she thought, she was a chain smoker herself. He finally got his way. He never stopped smoking after that day. Four years later she got a call at work that her husband had collapsed at her mother-in-law’s home. By the time they got to him it was too late. He had died of a sudden and totally unexpected heart attack. She has little doubt that his last four years of smoking was a major contributing factor to his sudden and premature death. So why was she now making such a big deal out of a cigarette? Once again, her own personal history was giving her a more powerful answer than I could ever have expressed. One cigarette, in a car a number of years earlier helped to end her husband’s life. If he had known the implication that one cigarette would have had, he would never have considered the thought for more than a second. In retrospect, she had the opportunity to look back to that day and realize how a fleeting urge followed by poor judgment helped to end or shorten her husband’s life. With the kind of personal experiences she had witnessed associated with smoking, it is quite easy to see how she could be so hard on herself for what occurred earlier that day. She witnessed how smoking diminished the quality of her father’s life and almost brought on a premature death. Equally important, she saw how quitting smoking vastly improved his health and general feeling of well being. She also witnessed how her husband’s momentary lapse of judgment resulted in her suffering such a grave loss just a few years earlier. If he had the opportunity, he would surely have cursed the day he lit just one. She had the benefit of hindsight, which now was haunting her because she had made the same mistake that day he had made just a few years earlier. He never got the chance to quit again. She still has time to make a decision—and she was asking me what she should do now. Again, I feel her own personal experience and the immediate emotional reactions she was now experiencing were giving a more powerful answer to her question than I could. If she listened to her heart, I am sure it was telling her to - NEVER TAKE ANOTHER PUFF!
|
|
Reply
| | | From: Joel | Sent: 7/12/2006 10:21 PM |
| | From: Joel | Sent: 2/8/2006 6:53 AM | | I just attached a few articles that address questions your have posed. As far as for checking in with your doctor, I always think it is a good idea for people to check in with their doctors after they have quit if they have questions or concerns, if for no other reason, than just for the peace of mind that everything seems to be okay from the doctor's perspective. I am going to attach an email response I sent to another person who had only smoked for three years, from about the age of 17 to about 20. He actually didn't tell me how many cigarettes he smoked per day. He wrote me when he was 23, saying that he hasn't really smoked in three years, "except" for maybe 5-10 cigarettes per year total. My response to him talked about the issue of pack years, which I think would be good for you to read. Generally, the number of pack years you have smoked is pretty low, at a level where most physicians would feel that if you were to never smoke again your risks would be negligible. The response went on to point out the greater risk he was dealing with, which was his not fully grasping the power of his addiction and the risk that future smoking was going to be posing for him if he did not come to grips with what he was still doing by his occasional smoking. Here is the response I wrote: The smoking that you have done to this point in time isn't really posing a major risk now. The way the calculate statistics showing real increases in smoking related illnesses is when measuring in " pack years." That is the number of years smoked being multiplied by the number of cigarettes you smoke per day. People generally have to have numerous pack years of smoking before the risks of smoking induced illnesses really go up significantly. Even then, if they quit before the onset of problems they begin to reduce their risks significantly. So generally, smoking as you did in the past probably is not posing a major risk to you now or in the future. Your greater concern needs to be on how you are minimizing the smoking you have done over the past few years. Not the risk of cancer or heart disease posed, but the risk of one day losing your quit and then ending up smoking for years and decades because you didn't fully appreciate or grasp the addictive nature of nicotine. The fact that you had ONE this year and not really wanting to count it is a major risk factor. This is a drug addiction and the next one or the next puff may hook you again. If you can, download and read the free e-book we have made available at HYPERLINK " http://www.whyquit.com/joel/ntap.pdf" www.whyquit.com/joel/ntap.pdf. It will clarify just what the risks of relapse is for people who minimize the concept of a puff. I think the book will help you to strengthen your resolve and help you to do the one thing that you can to really minimize your reasons for worrying--for it will make it clear that all you need to do now to reduce your risks of ever having to deal with the risk of another cigarette causing you any problems is to stick to your personal commitment to never take another puff. Joel | |
|
Reply
| | | From: Joel | Sent: 7/12/2006 10:23 PM |
Smoking's Impact on the Lungs
Ex-smokers are often tempted when watching others smoke. Spending time with a specific friend and watching them smoke may be a trigger especially if it was the most time you had spend with the friend since you quit smoking. The first time you have any new experiences, even if smoking is not part of the ritual, the thought for a cigarette will seem like a natural part of the ritual. Another factor is when watching a person smoke, the natural tendency is for the ex-smoker to start to fantasize about how good a cigarette will be at that given moment. A more productive way to handle the situation though is to really watch the person smoke one, and then wait a few minutes as they light another and then another. Soon you will see that they are smoking in a way that you don't want to and probably in a way that they don’t want to either. But they have no choice. You do. I am attaching a letter here that addresses this issue. It is a little harder to describe because it is based on a demonstration I do at live seminars. One demonstration I do at all my live seminars is a little smoking contraption made out of a plastic Palmolive bottle with a mouth piece inserted to hold a cigarette. The simulation shows how much smoke comes in when a person inhales, and how much comes out when they exhale. Smokers often feel they take in smoke and then blow most of it out, when in actuality, a very small percent actually comes out (about 10%). I always use cigarettes given to me by people in the audience, if I used one I brought people would think I was using a loaded cigarette. Anyway, below is a letter I wrote for clinic graduates who have seen this demonstration but the concepts apply to those who haven’t also. Viewing smoking as it really looks will minimize the temptation for even a puff. The letter is as follows ...
Whenever you watch a person smoking, think of the Palmolive bottle demonstration you saw the first day of the Stop Smoking Clinic. Visualize all of the smoke that goes into the bottle that doesn't come out. Also, remember that the smoker is not only going to smoke that one cigarette. He will probably smoke another within a half-hour. Then another after that. In fact, he will probably smoke 20, 40, 60 or even more cigarettes by the end of the day. And tomorrow will be the same. After looking at cigarettes like this, you don't want to smoke a cigarette, do you? I always suggest that clinic participants follow this simple visualization exercise to help them overcome the urge for a cigarette. When I suggested it to one participant who was off for three days she replied, "I see, you want me to brainwash myself so that I don't want a cigarette." Somehow I don't consider this technique of visualizing smoking brainwashing. It is not like the ex-smoker is being asked to view smoking in an artificially horrible, nightmarish manner. To the contrary, I am only asking the ex-smoker to view cigarette smoking in its true light. The Palmolive bottle demonstration accurately portrays the actual amount of smoke that goes in as compared to the small amount that you see the smoker blow out. Most smokers believe they exhale the majority of smoke they inhale into their lungs. But, as you saw by the demonstrations, most of the smoke remains in the lungs. When you visualize all the smoke that remains, it does not paint a pretty picture of what is happening in the smoker. Maybe not a pretty picture, but an accurate one. When an ex-smoker watches a person smoke a cigarette, he often fantasizes about how much the smoker is enjoying it--how good it must taste and make him feel. It is true he may be enjoying that particular cigarette, but the odds are he is not. Most smokers enjoy a very small percentage of the cigarettes they smoke. In fact, they are really unaware of most of the cigarettes they smoke. Some are smoked out of simple habit, but most are smoked in order to alleviate withdrawal symptoms experienced by all smokers whose nicotine levels have fallen below minimal requirements. The cigarette may taste horrible, but the smoker has to smoke it. And because the majority of smokers are such addicts, they must smoke many such cigarettes every single day in order to maintain a constant blood nicotine level. Don't fantasize about cigarettes. Always keep a clear, objective perspective of what it would once again be like to be an addicted smoker. There is no doubt at all that if you relapse to smoking you will be under the control of a very powerful addiction. You will be spending hundreds of dollars a year for thousands of cigarettes. You will smell like cigarettes and be viewed as socially unacceptable in many circles. You will be inhaling thousands of poisons with every puff. These poisons will rob you of your endurance and your health. One day they may eventually rob you of your life. Consider all these consequences of smoking. Then, when you watch a smoker you will feel pity for them, not envy. Consider the life he or she is living compared to the simpler, happier, and healthier life you have had since you broke free from your addiction. Consider all this and you will - NEVER TAKE ANOTHER PUFF!
A picture of the Palmolive Bottle Demonstration 
This looks like it was an exhalation after about 10 previous exhalations, not that much is seen in this particular photo. I normally get a tremendous amount of smoke out of the bottle with every drag, normally we can smoke up a room with one cigarette. If you look at the mouthpiece of the bottle, it is almost solid brown with tar. It used to be clear. I have used this bottle with somewhere between 300 and 400 cigarettes. While that may sound like a lot, most people smokemore than that in any given month. Even the bottle is pretty yellow and I blow out almost all of the smoke used when it inhales. The bottle is dry allowing me to do this, your lungs are moist trapping most of the tars when inhaled. Literally over 90% of the tar that is inhaled stays in the lung, when you see a person exhale they are literally blowing out about 10% of the smoke. You can see how the smoke had darkened the bottle after about a few hundred cigarettes. You can start to see how the smoker’s lungs below became so discolored. Smokers don't just put a total of a few hundred cigarettes in their system; they literally deliver hundreds of thousands of cigarettes over their shortened lifetime. This discoloration effect is more than just aesthetically unpleasant--it is in fact deadly. 
Above: Normal city dwellers lung.
Note black specks throughout indicative of carbon deposits from pollution.
Compare this to the lung below. 
Smokers lung with cancer. White area on top is the cancer, this is what killed the person. The blackened area is just the deposit of tars that all smokers paint into their lungs with every puff they take. To add a little more perspective to the demonstration, here is another way to see how much tar actually gets into the lungs from smoking. Below is the picture of a smoking machine. 
This machine smokes 2,000 cigarettes a day, mimicking smokers puffing patterns to capture equivalent amounts of tar as would a smoker. In one day the machine captures the amount of smoke in the picture below. 
The bottle above with the tar collected from 2,000 cigarettes. If a diluted form (diluted, not concentrated is as often done in animal experimentation to demostrate that chemicals are carcinogens) of this tar is painted on the skin of mice, 60% of the animals developed cancer of the skin within a year. 
Many chemicals currently banned for human consumption were removed from usage if they even caused 5% or less cases of cancer in similar experiments. Cigarette tars contain some of the most carcinogenic chemicals known to man. Consider this when watching people smoking and exhaling only 10% of the tars they actually take in. Not only are these chemicals being painted into the lung, but smoker are also constantly painting them up on their lips, tongue, larynx, swallowing some and thus painting it in the esophagus and throughout the digestive tract. Smokers have increased incidents of cancer in all of these exposed sites. Now that you know what it looks like on a large scale and feels like, lets take a look at the microscopic level of things that happen in the lung from smoking. The following series of slides illustrate microscopic changes that happen when a person smokes. The first slide is showing an illustrated blow-up of the normal lining of the bronchus. 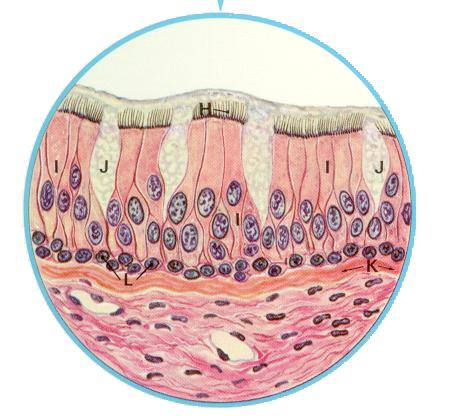
On the top we see the cilia, labeled (H). They are attached to columnar cells, labeled (I). The cilia sweep the mucous produced in the goblet cells, labeled (J) as well as mucous coming from deeper glands within the lungs and the particulate matter trapped in the mucous. The bottom layer of cells, labeled (L) are the basal cells. Below we start to see the changes that occur as people begin to smoke. You will see that the columnar cells are starting to be crowded out and displaced by additional layers of basal cells. Not only are fewer cilia present but the ones that are still functioning are doing so at a much lower level of efficiency. Many chemicals in tobacco smoke are toxic to cilia, first slowing them down, soon paralyzing them all together and then destroying them. 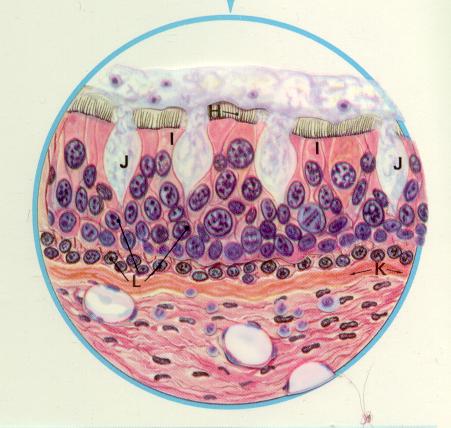
As you see with the cilia actions being diminished, mucous starts to build up in the small airways making it harder for the smoker to breathe and causing the characteristic smokers cough in order to clear out the airways. Eventually though, the ciliated columnar cells are totally displaced. As can be seen below ominous changes have taken place. Not only is the smoker more prone to infection from the loss of the cleansing mechanism of the cilia, but these abnormal cells (O) are cancerous squamous cells. These cells will eventually break through the basement membrane wall and invade into underlying lung tissue and often spread throughout the body long before the person even knows they have the disease. 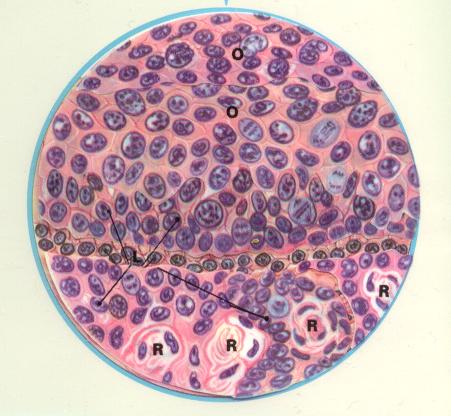
If a smoker quits before cancer actually starts, even if the cells are in a precancerous state, the process is highly reversible. Cilia regeneration starts in about 3 days once smoking stops. Even if cilia has been destroyed and not present for years, the lining tissue of the windpipe will start to repair. Even the precancerous cells will be sloughed off over time, reversing the cellular process to the point where the lining tissue goes back to normal. But if a smoker waits too long and cancer starts, it may be too late to save his or her life. Following are actual pathological slides showing these same damaging effects. 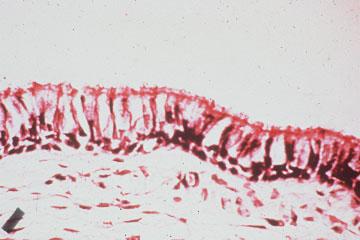
The little pink hairlike projections on the top is the cilia and if you compare this image with the illustrations above you should be able to see the mucous secreting cells and the separation of the lining tissue from the underlying lung tissue. Below you can see the same area of tissue from a smoker's lung who has totally destroyed the cilia in this tissue. 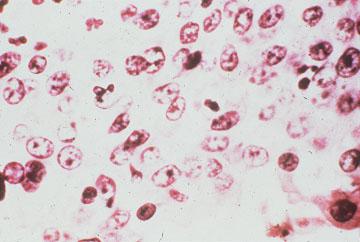
Again note, where there used to be two layers of well formed and orginized basal cells, now numerous layers of disorganized squamous cells has replaced the normal defensive tissue. These cells are precancerous and if the continued irritation (cigarette smoke) is not ceased can go to that final stage where they become malignant and invade into the underlying lunng tissue as seen below. 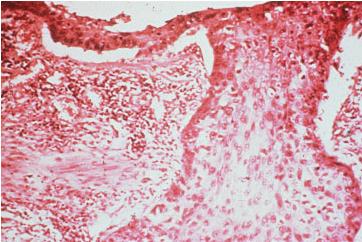
Then it is only a matter of time before it leaves the lung and spreads throughout the body. If the smoker quits smoking before this last cellular change occurs, before a cell turns malignant, the process seen in this last slide can be avoided. In fact much of the damage seen in the second picture here is highly reversible. In three days cilia start to regenerate and usually within 6 months the normal cilia function is returned. Also over time, the extra layers of cells will be sloughed off and the lining tissue of the bronchus will return to normal. Unfortunately, if a smoker waits until a malignancy has started, the outlook is grim. The overall 5 year survival rate for lung cancer is only 14%. Lung cancer, is a disease that while once uncommon, is now the leading cancer killer in both sexes. Cancer is actually many different diseases with many different causes. If we look at cancer trends over the last century we see some amazing changes. While cancer was always around, it was different sites that were primary problems. Lung cancer, at the turn of the century was almost unheard of. If a doctor saw a case he would have easily gotten it printed up in a medical journal. Now, it is the major cause of cancer death in our society, killing more men and women than any other site. The primary difference between now and then is smoking. Before the turn of the century smoking was a limited practice. A very small percentage of people smoked and even the ones who did smoked many fewer cigarettes. Cigarettes were not even mass produced till the very end of the 1900’s. We always hear of a cancer epidemic, how more and more people die of cancer every year. Actually, if you pull the smoking related sites out of the equation, cancer deaths have been on a decline. Some sites, like stomach the incidence dropped dramatically, not fully understood as to why. Other sites, like breast, even though the morbidity rate (number of cases) didn't drop, because we now have better treatments and earlier detection, the mortality (death) rate has dropped. But the smoking cancers; lung, mouth, lip, tongue, throat, larynx, pancreas, esophagus, pharynx, urinary bladder have all seen marked increases over the 20th century. These cancers have gone from obscurity to some of the major causes of death in our country. Actually, for the first time in a hundred years we are starting to see an early decline of morbidity and mortality because we are seeing fewer smokers now with the drop in the percentages of adult smokers. 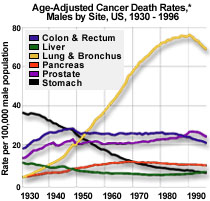
Men
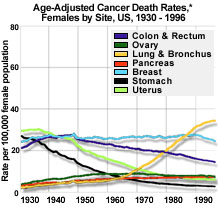
women
You see a dramatic difference in men and women, especially in lung cancer rates. The reason is women started smoking much later than men, about a 30 year time delay before it became socially acceptable for women to smoke. Male smoking rate jumped dramatically between World War I and another big boost during World War II. Free distribution of cigarettes to soldiers was a big factor. Women smoking rates happened much later and the time delay is reflected in the time delay in cancer and otehr diseases going up too. The above pictures were primarily about how smoking causes cancer of the lung and other sites. But the assault on the lungs from the tars in tobacco are not just limited to causing cancer. Other lung diseases are directly caused by smoking, the most well known are the chronic obstructive lung diseases. The most well known smoking induced COPD is emphysema. This is another one of those diseases that primarily happen to smokers. Over 90% of the cases are smoking induced. There are cases in some families where there does seem to be a genetic predisposition, where non-smokers get it too. This is from a rare condition, a lack of a blood enzyme called alpha1antitrypsin. This again is rare, but if you do have family members who never smoked a day in their life get emphysema there may be a genetic tendency. But again, over 90% of emphysema cases are simply caused by smoking. Eradicate smoking and you eradicate the risk of the disease. To get a sense of how a long is altered by smoking to cause emphsema look at the pictures below. The first is a picture of an inflated non-smoker city dweller's lung. 
As in the normal picture of a lung above, you can see carbon deposits collected throughout from pollution effects. But when contrasted with a smoker's lung with emphysema... 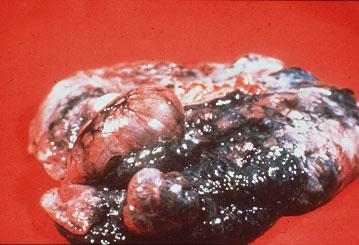
...there is a very dramatic visible difference. Not only is the discoloration the issue, but the lungs have literally been ripped out of shape making breathing extremely difficult and eventually impossible. To get a sense of what it feels like to breathe with emphysema take a deep breath and hold it. Without letting out any air, take another deep breath. Hold that one too. One more time, take one more breath. Okay let it all out. That second or third breath is what it feels like to breathe when you have advanced emphysema. Emphysema is a disease where you cannot exhale air. Everyone thinks that it is a disease where you cannot inhale but in fact it is the opposite. When you smoke you destroy the lungs elasticity by destroying the tissue that pulls your lung back together after using muscles that allow us to inhale air. So when it comes time to take your next breath it is that much more difficult, for your lungs could not get back to their original shape. Imagine going through life having to struggle to breathe like those last two breaths I had you take. Unfortunately, millions of people don't have to imagine it, they live it daily. It is a miserable way to live and a slow painful way to die. Hopefully when you breathe normally today you are not in pain and you are not on oxygen. If you don't smoke you will continue to give yourself the ability to breathe longer and feel better. Never lose sight of this fact. To keep your ability to breathe better for the rest of your life always remember to - NEVER TAKE ANOTHER PUFF!
Joel
© Joel Spitzer 2001
Page last updated by Joel Spitzer on August 25, 2003
How does smoking impact circulation? 
|
|
Reply
| | | From: Joel | Sent: 7/12/2006 10:25 PM |
Smoking and Circulation
While most people equate smoking deaths to cancer and lung disease, in fact many more people will die from circulatory conditions from smoking than die from cancer or other lung diseases. Also, in general, they will die at much younger ages from these problems. We would have many more lung cancers than we do if smokers could live long enough to get them. When many people with fatal heart attacks or strokes are autopsied, there are often precancerous lesions found that indicate that if these people had a few more years to live they would have eventually succumbed to these smoking induced diseases. As for heart and other circulatory diseases, the two chemicals in cigarette that stand out as the biggest problems are nicotine and carbon monoxide. Nicotine, besides being addictive, has very powerful effects on arteries throughout the body. Nicotine is a stimulant, speeding up the heart by about 20 beats per minute with every cigarette, it raises blood pressure, is a vasoconstrictor which means it makes arteries all over the body become smaller making it harder for the heart to pump through the constricted arteries and it causes the body to release its stores of fat and cholesterol into the blood. The heart has to work harder to overcome all of these effects. To work harder the heart, like every other muscle in the body, needs extra amounts of oxygen for the additional workload. The oxygen has to be transported through the blood. But carbon monoxide from tobacco smoke literally poisons the oxygen carrying capacity of the blood. So this results in the heart having to work harder to get more blood to itself to work harder, because it's working harder. This is a circle. A vicious and deadly circle when it comes down to it. Below we see the cross section of a normal artery. Usually we have nice big openings in the artery to carry oxygen as well as all other nutrients to all the tissues of the body. 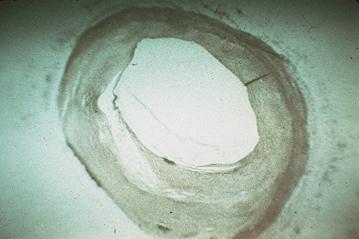
If you compare this artery to the one below... 
You can see the blood clotted blocking the blood flow to whatever organ or tissue this artery was leading to. Without being able to get circulation, that tissue will literally suffocate in a matter of minutes and basically be left as useless tissue. Sometimes the artery involved is a coronary artery, one that supplies the heart with the blood it needs to function. Below is a picture of a coronary artery attached to the heart... 
If we look at a close up view of the artery... 
Here we see the blood clotted and blood flow to the section of the heart that this artery was supplying was cut off. What will result is that a portion of the heart muscle that was supposed to get that blood flow suffocates and dies within a matter of minutes. 
Above we see infarcted (dead) heart muscle (myocardial infarction). The tissue is literally brittle as illustrated by the cracking effect. Instead of being able to pump blood, this area whole section of muscle is no longer able to be utilized for its life sustaining function. Again, smokers get this much more often because of the effects of nicotine and carbon monoxide. Nicotine having all the direct effects on the heart itself, carbon monoxide robbing the oxygen supply, and both chemicals increasing clotting as well as clogging factors in the blood. If the section of the heart affected was larger enough the smoker would die from the first attack. Often smaller areas are affected and the patient can survive but has lost that specific section of the heart and may have permanent impairments from the now limited supply of heart tissue. Cigarette smoking increases risks of blood clots significantly. If the blood clots in an artery and blood can no longer get through, the tissue that is supposed to be supplied with blood has lost the source of its oxygen and nutrients and dies in minutes. But clots are not the only way these arteries can be blocked. Another way is by clogs. As opposed to clots where the blood actually coagulates and becomes an obstruction, clogs are where deposits of fat gradually build up. In the first picture below you can literally see the start of a artery getting a fat buildup. 
Over time, this opening can get narrower and blood flow gets more and more impeded. This of course adds to the workload of the heart to pump through smaller arteries with increased resistance. But this clogging does not only happen to the coronary arteries, it literally happens all over the body. Remember, nicotine is not only a vasoconstrictor, making arteries go into constrictions every time it is administered, but it also causes the body to release its own stores of fat and cholesterol. Besides this, carbon monoxide has an effect that makes the fat stick to the arteries. The reason is carbon monoxide lowers the oxygen level of the blood (hypoxia) and hypoxia seems to have an effect making fat stick to artery walls. Eventually over time arteries can become totally blocked with fat as seen in the slide below. 
As in the case with a clot, blood cannot get through and the body part that was contingent on that blood supply for survival is lost. If this artery lead to your heart as in the case of the clotted coronary arteries above, the result would be a heart attack with a loss of heart muscle that if large enough would be fatal. But the heart is not the only organ affected this way. Another common site of problems are the arteries leading to the brain. Below is a picture of the base of a health human brain. 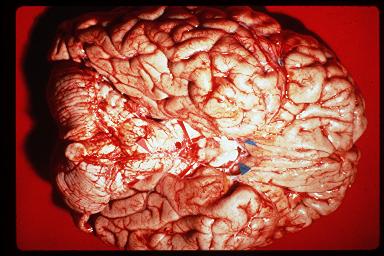
The arteries to the brain are very small here and clear, very difficult to see in fact. The arrows are pointing them out. To see them clearer here is a close up shot of these arteries... 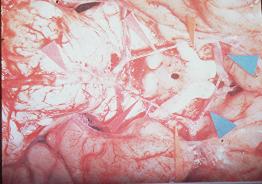
Again note, these arteries are very thin and clear. Smoking increases the fat deposits to these arteries so often, instead of looking like this, they can look like the slide below... 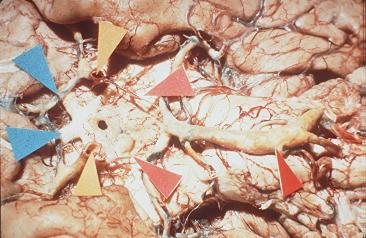
With the fat build up the arteries are much easier to see. But this build up if complete cuts off circulation to your brain and as is the case with the heart, the part of the brain that no longer gets circulation dies. This is what happens in the case of a stroke. Circulation gets cut off from the brain either through a clog or a blood clot. The section of the brain that gets cut off suffocates and dies. If this part of your brain controlled speech, you will not talk anymore, if it controlled some form of motor function, these abilities will be lost and leave the patient impaired or crippled. If the section of the brain affected controlled some life sustaining function, the patient will die, again, within minutes of when the circulation cut off is complete. The clogging and clotting effects of nicotine and carbon monoxide are the primary reasons why smokers are at such a higher risk of this condition. But this clogging/clotting effect is not limited to just major organs like the heart or brain. These chemicals affect arteries throughout the entire body. These affects may not be as deadly as cutting off circulation to the heart or brain, but in a real way they can show the true potential of the grip of the nicotine addiction. Peripheral circulation, arteries going to the extremities are also highly susceptible to the vasoconstrictor effects of nicotine as well as the increase of clots and clogging risks posed by smoking. Smoking is a primary cause of much of the peripheral vascular disease seen as well as a powerful aggravating factor for people who have other preexisting conditions causing circulation problems to the extremities. One condition though stands out as being truly unique and in many ways, demonstrates the real addictive nature of nicotine better than any other cause. The condition is known as Buerger’s Disease (thromboangiitis obliterans.) Buerger’s Disease is a condition where there is a complete cutoff of circulation to the finger or toes, resulting in gangrene. 
Once gangrene occurs the only course of action is to amputate the affected area. 
The most common age bracket that this disease strikes is in people between the ages of 20 to 40, normally young to get circulation problems that result in amputations. While it is much more common in men, women are affected to. What makes Bueger’s Disease unique is that it is a disease that is basically exclusive to smokers. There are almost no documented cases of this disease happening in a non-smoker. Smoking is the primary etiologic factor. This is a rare disease, but noteworthy because of this unique nature of happening only in smokers. If a smoker gets lung cancer, the person and other people can sometimes think, “well non-smokers sometimes get lung cancer too, maybe cigarettes didn’t cause it.�? Same thing with heart attacks or strokes, non-smokers get them too, smokers just get them much more often. But again a certain level of denial can be exhibited and there is no way to conclusively prove that cigarette did it. But Buerger’s Disease, having no other known cause and basically never happening in non-smokers does not lend itself to such denials. When a doctor determines he or she is dealing with a Buerger’s Disease patient, a basic ultimatum is going to be delivered—quit smoking or lose your limb—your choice! If we were dealing with simply a bad habit, how many people given such an ultimatum and knowing it is true would continue doing the particular behavior given such consequences? While Buerger’s Disease is much more common in men, I have personally had two women who were Bueger’s Disease patients in my clinics. My first actual encounter with a Buerger’s Disease patient was with a woman who was 38 year old when I met her, which was about 24 years ago. Three years before I met her, at the age of 35 she was diagnosed with Buerger’s Disease. This is actually relatively late to first be diagnosed. Her doctor had told her she had to quit smoking, but she did not comply and within a few months she had her right leg amputated. The circulation in her left leg was also badly affected, and after the hospitalization from the amputation she did quit smoking and had no further circulatory complications for the next three years. Then one night at a party, a friend offered her a cigarette. She figured that since she had been off cigarettes for so long, she now had control over her habit. If she liked the cigarette, she would smoke one or two a day. If she didn't like the cigarette, she just wouldn't smoke anymore. Well, she took the cigarette. She didn't particularly like the cigarette, but the next day she was up to her old level of consumption. Four days later she lost circulation in her left leg. She knew the reason. After three years with no problem and only four days after going back to smoking her circulation was affected. Her doctor told her that if she did not quit immediately, she would probably lose her other leg. This is when I met her. She enrolled in a smoking clinic that week and quit smoking. Almost immediately her circulation improved. The doctor took her off anti-coagulant drugs and vasodilators he had put her on a few weeks earlier to try to slow up the process even though they were highly ineffective at stopping the likelihood of gangrene and amputation. But once she quit smoking she no longer needed them. Soon, her circulation was back to normal. Nine months later, I called to ask her to serve on a panel. At that time, she sluggishly replied, "I can't come. I have been in the hospital the last two months." When I asked what had happened, she hesitantly replied, "I had my toes amputated." She had gone back to smoking. She tried one because she just couldn't believe she would get hooked again. She was wrong. She lost circulation, had her toes removed and eventually had her leg amputated. I have had other clinic participants with similar experiences, being told to quit smoking or lose limbs who did not quit smoking. The reason I talk about this particular woman again and again is about a year after she had the second amputation, she came back into a clinic I was conducting and told me she had quit again and was now off about 9 months. I told her I was surprised, I thought she had permanently lost control. After all, she had her leg removed, the toes from her other foot, and eventually her second leg. When I confronted her with that information she replied, "The doctor finally convinced me. He said, 'You might as well keep on smoking, I'll just take your arms off next.'" That scared her into quitting smoking. Her next comment to me was unbelievable. She looked me straight in the face, dead seriously, and said "I DIDN'T NEED A HOUSE TO FALL ON ME TO TELL ME TO QUIT SMOKING." I had periodic contact for the next 15 years at which time she moved away. She was fine over that whole time period. Whenever I brought up that conversation, we both found ourselves amazed that she could ever have made such an irrational statement. She happened to be a very rational, bright and inspirational individual. She would get around on wooden legs, socializes, and even occasionally would sing and dance on stage. Once she had broken free of the drug's effects and the smoker's psyche, she knew she could do anything. Frequently, I would encounter people who quit smoking on their own. When I ask how they did it, they tell me of this marvelous lady they met who told of how she used to be hooked on smoking. Hooked so bad, in fact, that she had her legs amputated from a smoking related illness. It usually turns out to be the same person. By spreading her story, she offers inspiration and hope to countless smokers to break the habit before the habit breaks them. Her story represents the real power of the addiction. She could not deny any where along the way smoking wasn’t the cause. Not only would every doctor and all the research she could do pinpoint smoking as what was causing her problem, but she had quit, was fine, relapsed and within days lost her circulation—twice! The second time she actually lost her toes and her foot and then her lower leg. There was absolutely no way she could deny the cause and yet it took another 9 months for her to quit again. Her continued smoking and ease of relapsing shows nicotine dependency at its worst. This overpowering nature of nicotine should not be lost on anyone here. You probably don’t have a condition that is obvious as to force you to make a decision almost immediately upon relapse. In many ways this is worse, for cigarettes are quietly and insidiously destroying you, sometimes with little warning, or at least ones you will acknowledge. The first symptom to many circulatory diseases caused by smoking is sudden death. You may get no second chance. Once you have a quit smoking, do everything in your power to make it last. You don’t know that you will have the desire, strength or worst of all, the opportunity to quit next time. A tragic and fatal disease may get you first. Always consider the full danger of smoking and power of the addiction and your likely choice will be to - NEVER TAKE ANOTHER PUFF! |
|
Reply
| | | From: Joel | Sent: 7/12/2006 10:27 PM |
Setting Quit Dates
Conventional wisdom in smoking cessation circles says that people should make plans and preparations for some unspecified future time to quit. Most people think that when others quit smoking that they must have put a lot of time into preparations and planning, setting quit dates and following stringent protocols until the magic day arrives. When it comes down to it, this kind of action plan is rarely seen in real world quitters. I emphasize the term real world quitters as opposed to people quitting in the virtual world of the Internet. People who seek out and participate in Internet sites do at times spend an inordinate amount of time reading and planning about their quits before taking the plunge. Even at our site we see people say they were reading here for weeks or months before finally quitting and joining up. Although I suspect there are a fair number of people who had already decided to quit right away and searched us out after their quit had begun, and some people who may not have actually decided to quit but who when finding WhyQuit.com and seeing cigarettes for what they are decided then and there to start their quits. Getting back to real world experience though, the best people to talk to when it comes to quitting smoking are those who have successfully quit and have successfully stayed off for a significant period of time. These are people who have proven that their technique in quitting was viable considering they have quit and they are still smoke free. Talk to everyone you know who is off all nicotine for a year or longer and find out how they initially quit smoking. You will be amazed at the consistency of the answer you get if you perform that little survey. People are going to pretty much fall into one of three categories of stories. They are: -
People who awoke one day and were suddenly sick and tired of smoking. They tossed them that day and never looked back. -
People who get sick. Not smoking sick, meaning some kind of catastrophic smoking induced illness. Just people who get a cold or a flu and feel miserable. They feel too sick to smoke, they may feel too sick to eat. They are down with the infection for two or three days, start to get better and then realize that they have a few days down without smoking and decide to try to keep it going. Again, they never look back and stuck with their new commitment. -
People who leave a doctors office who have been given an ultimatum. Quit smoking or drop dead--it's your choice. These are people for whom some sort of problem has been identified by their doctors, who lay out in no uncertain terms that the person's life is at risk now if they do not quit smoking. All of these stories share one thing in common--the technique that people use to quit. They simply quit smoking one day. The reasons they quit varied but the technique they used was basically the same. If you examine each of the three scenarios you will also see that none of them lend themselves to long-term planning--they are spur of the moment decisions elicited by some external circumstance. I really do encourage all people to do this survey, talking to long- term ex-smokers in their real world, people who they knew when they were smokers, who they knew when they quit and who they still know as ex- smokers. The more people do this the more obvious it will become how people quit smoking and how people stay off of smoking. Again, people quit smoking by simply quitting smoking and people stay off of smoking by simply knowing that to stay smoke free that they must never take another puff! Joel © Joel Spitzer 2006 Page created February 19, 2006 and last updated by Joel Spitzer on February 19, 2006
The British Medical Journal reported an interesting study that tied into this article very well. Here is a link to the abstract of that study: http://bmj.bmjjournals.com/cgi/content/abstract/bmj.38723.573866.AEv1 I wrote a reply to the journal that got posted on their response website. Here is a link to that reply: http://bmj.bmjjournals.com/cgi/eletters/bmj.38723.573866.AEv1#127706 That commentary elicited a reply from another person, who was basically trying to give the impression that serious scientists shouldn't put too much emphasis on real world experiences. I wrote a reply to this editorial but it somehow did not seem to get past the editorial review board at the British Medical Journal. I think the reply is still valid so I am attaching it below:
|
| | Joel Spitzer,
Health Educator
Conduct Stop Smoking Clinics for the Evanston and the Skokie Illinois Health Departments 60201,60076 Send response to journal:
Re: Re: Flawed reasoning
| "...because something commonly happens in a particular way 'in the real world' then this should be considered the best way." Smoking cessation experts often seem to have to be telling people to dismiss real world experiences. Usually I see a little different variation of the comment above. Common statements I have seen are something to the effects that while it is likely that a person may at times encounter real world quitters who succeeded by using non-recommended techniques, usually meaning no pharmaceutical intervention or in what this study is showing, people who used no set quitting date, that these people are just the exceptional cases. What the experts are trying to do in effect is discredit observations made by people, making them think that the occurrence of such experiences are really rare. The author above was at least accurate enough to say, "While it is true that most smokers who quit do so without any specific behavioral support or pharmacological treatment..." The rest of the comment was going on to try to give the impression that there would have been even more successful quitters if people would just do what smoking cessation experts say should work as opposed to doing what actual quitters continually say has worked for them. The tactic being employed here is to leave the impression that we could just have a whole lot more successful quitters if people would just utilize the miraculous effective products out there that actually help people to quit. There is also the perception being portrayed that there really are very few ex-smokers out there because most who have tried to quit have done so unaided and everyone just knows how improbable it is for people to be able to quit in an unaided attempt. Medical professionals and the general public are being misled to believe that quitting smoking is just too plain difficult for people to do on their own and that the odds of a person actually quitting on their own is really pretty dismal. This would all make perfect sense if not for the fact that we have so many successful ex-smokers in the real world. In America, we have more former smokers than current smokers. Over half of the people who used to smoke have now quit smoking. From the comment made above it should be clear to all that most of the people who have quit either did not know of professional recommendations for quitting or chose to ignore professional intervention techniques. Yet these people successfully quit anyway. I think that this is an important point to hit home with all medical professionals. The medical profession has got to start to help people to realize the real potential of success that individuals do have to quit smoking instead of perpetuating the idea that quitting is just too hard for an individual smoker to expect to actually succeed without help. While this article should have been about planning techniques, the original author and a few experts weighing in on the discussion have tried to turn it into a referendum on selling pharmaceutical interventions. Nicotine replacement products have been around for over two decades now-- and a significant percentage of smokers have used them to try to quit smoking. If a product has been around for decades, used by millions of people worldwide, AND, has been truly effective, it should be easy for most health care practitioners to come up with lots and lots of successful patients, colleagues, family members and friends who have quit with these products. As I said in my original commentary above: " I don't believe that there is a single professional smoking cessation "plan your quit" advocate who will suggest other medical professionals should take a similar survey. For if they did their study results would almost certainly be called into question when the health care professional starts seeing the results of his or her real life survey. The experts will end up having to spend quite a bit of time trying to explain away the discrepancy, using rationalizations like the people who planned their quit "didn't do it right" or didn't "plan" long enough or were "just more addicted smokers." In all honesty, I don't expect my encouraging of real world observations by health care professionals to have much impact with smoking cessation experts. They are going to profess to believe whatever other experts keep telling them to believe or, what the funders of their studies believe. I do however believe that health care workers who are on the front line and actually deal with patients who smoke are going to be a bit more critical and analytical about this. If they spend any time talking with patients they are going to see through the rhetoric and the rationalizations of the experts. I have always tried to disseminate the message that just because something works in the lab or in study conditions doesn't necessarily translate to the fact that the process will work in the real world. The smoking cessation experts seem to have to work on the basis that just because something works in the real world doesn't mean that it is a good approach if it doesn't seem to work in a lab. I have high hopes that medical professionals really wanting to help their patients are going to be more influenced by what they see is successful than by being told by the experts what should be successful, but somehow not replicable in their own practices. | |
|
Reply
| | | From: Joel | Sent: 7/12/2006 10:28 PM |
| | | From: Joel | Sent: 3/8/2006 4:03 PM | Most people, when thinking of smoking risks only think of diseases directly caused by smoking. But smoking can play a major risk in treating diseases and injuries that in a true sense are not caused by or have anything to do with smoking. I am referring to the risk of postoperative complications.
Many doctors will hold off doing elective or non-essential surgeries for as long as possible in order to give a patient time to be totally smoke free. This is not a practice done for arbitrary reasons. Surgery is much riskier to perform on a smoker.
Your risks of complications of anesthesia or postoperative complications are much higher while you smoke. These complications can be serious, making you suffer much longer and possibly putting your life at risk. The longer you are off prior to surgery, the lower the risk becomes.
One cardiologist I worked with in smoking cessation programs over 25 years ago studied the risk of postoperative complications at the hospital where he was then chief of cardiology and thoracic surgery.
At that time he found that in non-smokers the postoperative complication rate was 1 in 50. Smokers had a rate of 1 in 3. If the surgeries were elective and they could wait for the patient to quit, he found that if the smoker would quit for just a week, the rates were 1 in 12. Of course it wasn’t as good as a person who had been off for years but it was far superior to current smokers.
The longer people were off the closer the rate became to non-smokers levels. The important thing is to quit as far ahead of any procedure as soon as possible. The only way to get maximal benefit of longest-term cessation prior to any future surgery is to stay smoke free today and for as long as you live remember a day at a time to never take another puff!
Joel | | Reply
| | | From: Joel | Sent: 3/8/2006 4:04 PM | For anyone who was planning on quitting at some future date but suddenly finds out that he or she may need an emergency surgery this week because of an ongoing smoking induced illness, or because of an sudden onset illness, or because of an accident or injury totally unrelated to your smoking. Your future quit date may do you no good at the time you needed it most, if that time is today. The day you quit smoking you instantly start to reduce your risk of post-operative complications and a host or other problems, and these risks continue to drop throughout your life if you simply stick to your commitment to never take another puff!
| | |
|
|
First
Previous
2-8 of 8
Next
Last
|
|
|

 Important Announcement
Important Announcement


 Return to General
Return to General